Needa Zalloum1,
Rana Abu Farha2 ![]() ,
Oriana Awwad1,
Nabil Samara3
,
Oriana Awwad1,
Nabil Samara3
For correspondence:- Rana Farha Email: r_abufarha@asu.edu.jo Tel:+6265609957
Received: 9 February 2016 Accepted: 3 October 2016 Published: 29 November 2016
Citation: Zalloum N, Farha RA, Awwad O, Samara N. Inappropriate prescribing of proton pump inhibitors among patients in two Jordanian tertiary health facilities. Trop J Pharm Res 2016; 15(11):2489-2495 doi: 10.4314/tjpr.v15i11.26
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To evaluate the current prescription pattern and appropriateness of proton pump inhibitors (PPIs) in two of the largest tertiary hospitals in Jordan, and also to determine their utilization rate among the admitted patients.
Methods: A retrospective cross-sectional study was conducted over 10 months (February-November 2013) at two Jordanian tertiary hospitals. A total of 193 patients, both in intensive care unit (ICU) and non-ICU, who were receiving PPIs prescriptions as part of their drug regimen during their hospitalization, were recruited. Patients were accessed from different hospitals’ wards (non-ICU and ICU) using a convenient sampling technique. The appropriateness of PPIs and the rationale for their prescription as a treatment or prevention therapy were evaluated according to the recent treatment guidelines.
Results: The results showed that PPIs were being overused; only 53 patients (27.5 %) were prescribed PPIs for a correct indication, while the remaining 140 patients (72.5 %) were receiving PPIs without any documented valid indication. By comparing the patients according to their site of care, 52.4 % (43/82) of ICU patients compared to 87.4 % (97/111) of medically hospitalized patient (non-ICU) were inappropriately receiving PPIs (p = 0.000).
Conclusion: Adherence to the current practice guidelines for safe prescription of PPIs is poor. Thus, updating physicians on the practice guidelines, participation of a clinical pharmacist in making therapeutic decisions and modifying hospital formularies are measures that would be helpful and thus contribute to improved healthcare in Jordan.
Introduction
Proton pump inhibitors (PPIs) are among the most commonly prescribed drugs worldwide [1]. They are a class of medications widely used to suppress gastric acid secretion; playing a central role in the management of different conditions such as duodenal and gastric ulcers, severe reflux oesophagitis, scleroderma oesophagitis, and Zollinger–Ellison syndrome [2,3]. They are also prescribed as a prophylactic treatment for stress ulcer in intensive care units (ICU) patients [4], in preventing gastric ulcers induced by non-steroidal anti-inflammatory drugs (NSAIDs) [5] and combined to antibiotic therapy as part of the eradication regimen of Helicobacter pylori in patients with peptic ulcer disease [6].
Nowadays, PPIs are considered the most potent gastric acid-suppressing agents available in clinical use; they are substantially more potent, longer-acting than H2-receptor antagonists and produce a faster, and more complete healing of oesophagitis as well as relieving of heartburn [7-9].
Although extensive clinical trials and post-marketing surveillance indicate that PPIs are safe and well tolerated, their use has been linked to a broad spectrum of adverse events affecting different body systems, such as increased risk of intestinal dysbiosis, specific infections, including pneumonia and Clostridium difficile infection, osteoporosis, nutritional deficiencies [10-12]. In addition, the cost of PPIs exceeds that of any other acid inhibiting medication and the volume of prescribing them has had a substantial impact on the medical bills worldwide [13,14]. In this regard, several reports have suggested that PPIs are being overused in hospital and ambulatory care settings [10,15,16], and that the appropriateness of PPIs prescriptions in some hospitals may be as low as 8.3 % [16]. Suggested causes contributing to the inappropriate overuse of PPIs include physician type, practice setting, formulary status and consumer-oriented advertising [17].
Based on this, the concept of overuse of these acid-inhibiting agents in the clinical practice has received significant attention; relative to both the potential for adverse effects and the preventable cost-expenditure. Indeed, studies spanning over a decade have demonstrated that physicians, in both primary and specialty care, may overprescribe these medications without re-evaluating patients for persistent clinical indication [10,15,16]. Thus, the main aim of this current study was to evaluate the current prescription status of PPIs in medical patients, this will help to establish a policy to ensure appropriate therapy prescription and minimizing the risk and non-judicious cost expenditure.
Methods
Study design, settings, and data collection
A retrospective cross-sectional study was carried out on patients treated at two of the busiest tertiary hospitals (Jordan university hospital and Jordan hospital) in Amman between February-November 2013. During the study period, 200 adult patients, who fulfilled the inclusion criteria, were approached, out of which 193 patients agreed to take part in the study (response rate 96.5 %). The inclusion criteria included adult patients (≥ 18 years of age) who were receiving any PPIs as part of their drug regimen started during their hospitalization. Patients were accessed from different hospitals’ wards (non-ICU and ICU) using convenient sampling technique.
Well-trained assistants, using a structured questionnaire, recruited the study sample. Information regarding demographic data, clinical characteristics, medical history, current medications, and risk for peptic ulcer disease i.e. use of NSAID, and stress-induced ulcer were collected and documented. Data were collected simultaneously from medical files and patients interview.
Ethical approval
The study was conducted following the ethical standards outlined in the World Medical Association Declaration of Helsinki guidelines [18]. All participants were required to provide a written informed consent. Ethical approval was obtained from both the University of Jordan (ref no. 1/23/2015/2016) and Jordan Hospital (ref no. 15/1/2013).
Determination of appropriateness of PPIs prescription
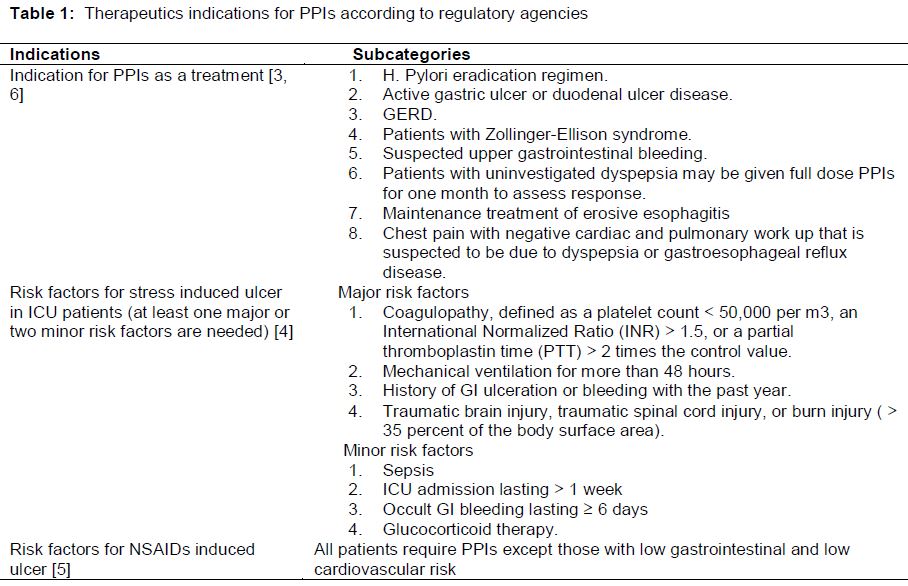
The appropriateness of PPIs and the rationale behind their prescription as a therapeutic and prophylactic agent were evaluated according to latest guidelines () [3-6]. Accordingly, patients were classified into four categories: 1) those receiving PPIs as a treatment for gastric-acid related disorders; 2) those receiving PPIs for prevention against stress-induced ulcer; 3) those receiving PPIs for prevention against NSAIDs-induced ulcer; and 4) those receiving PPIs for no clear therapeutic indication.
To assess NSAIDs-induced ulcer risk, both the cardiovascular and gastrointestinal risks were evaluated [5]. Except for those at low cardiovascular and low gastrointestinal risk, all patients on NSAIDs require the addition of PPI therapy. Risk for stress-induced ulcer was assessed by evaluating the presence of majors and minors risk factors, if any patient has at least one major or two minor risk factors, then PPIs should be initiated [4].
Statistical analysis
All data were entered and analyzed using SPSS© 19 (SPSS, Inc., Chicago, IL, USA). Categorical variables were expressed as frequencies and percentages, while continuous variables were presented as means ± standard deviation (SD). Normality of the data was determined using the different normality indicators (skewness and kurtosis). Chi- Square test was used to evaluate difference between groups for categorical variables. For all statistical analysis, p < 0.05 was considered statistically significant. All tests were two-tailed.
Results
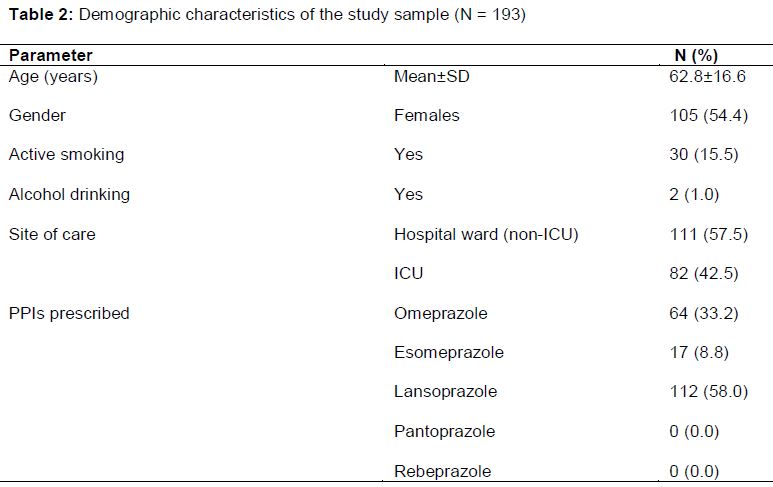
The demographic details of patients included in this study are presented in . The mean age was 62.8 years and around 42.5 % (82 patients) of patients were ICU patients. Women accounted for 54.4 % (105 patients) of all the patients recruited. At present, there are five PPIs available in Jordan: omeprazole, lansoprazole, pantoprazole, rebeprazole and esomeprazole. Lansoprazole was the most commonly prescribed PPIs (112 patients, 58.0 %), followed by omeprazole (64 patients, 33.2 %) and esomeprazole (17 patients, 8.8 %). Pantoprazole and rebeprazole were not prescribed at all.
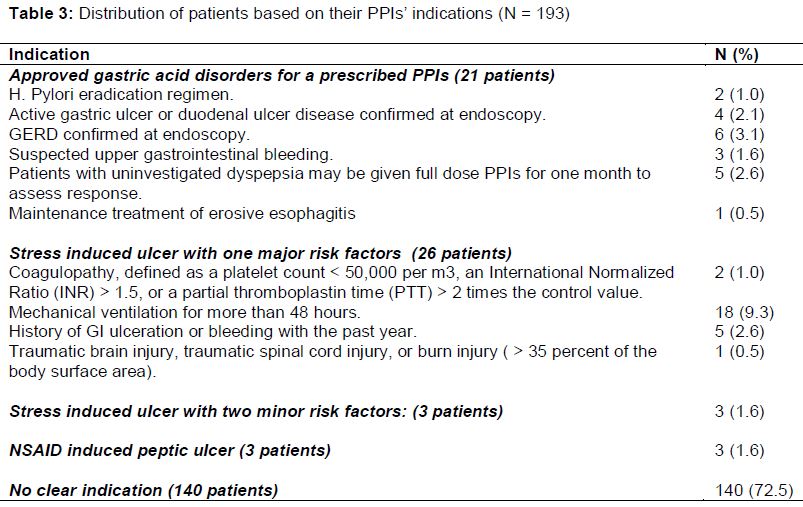
The appropriateness of PPIs prescription among study sample was assessed by taking into account the indications and risk factors mentioned previously in . showed that only 27.5 % of patients (53 patients) have received a proton pump inhibitor for valid indications. When stratifying patients according to their site of care, 52.4 % (43/82) of ICU patients compared to 87.4 % (97/111) of medically hospitalized patient (non-ICU) were found to receive PPIs for no valid medical indication (p = 0.000).
Among patients with valid indications, 21 patients (10.9 %) have approved gastric acid disorders, 29 patients (15.0 %) were at risk for stress-induced ulcer, while only 3 patients (1.6 %) were at risk for NSAIDs induced ulcer. It is obvious that mechanical ventilation for more than 48 hours was the most common risk factor encountered (18 patients, 9.3 %).
On the other hand, when looking at the patients on PPIs with no clear indications, investigation of reasons behind inappropriateness of PPIs prescriptions showed that 51 patients (36.4 %) were on PPIs because they were concomitantly receiving low dose of aspirin without other risk factors for gastrointestinal tract bleeding. Other subsequent reasons behind inappropriate PPI use were; use of corticosteroids (20 patients, 14.3 %), use of low molecular weight heparin (30 patients, 21.4 %); use of warfarin (7 patients, 5.0 %), and use of unfractionated heparin (4 patients, 2.9 %). Regarding the remaining 28 patients (20.0 %), there were no documented indications reported in patients’ medical records.
Discussion
PPIs comprise a cornerstone in the management of a vast plethora of gastric acid associated conditions. Although they are considered a safe and effective group of pharmaceutical agents, their use is not void of serious adverse events [10-12]. Using PPIs safely requires striking the current guidelines and recommendations issued by regulatory agencies [3-6]. As recommended by recent guidelines, PPIs are prescribed only for patients with approved gastric acid disorders as well as for prevention of stress and NSAIDs induced ulcer. Unfortunately, there is a growing body of evidence that there is a dramatic increase in PPIs overuse in hospital and ambulatory care settings that is associated with certain health hazards, and lead to an unnecessary waste of hospital resources as well as overall health system resources [10,15,16]. Whether guidelines recommendations are being followed or implemented in clinical practice was generally unknown in Jordan.
Lansoprazole was the most commonly prescribed PPIs among study patients. Despite the fact that all PPIs are equally effective at appropriate recommended doses, pantoprazole and lansoprazole appear to have a less significant potential to provoke any significant drug-drug interactions if compared to esomeprazole or omeprazole [19]. Identification of the most commonly prescribed PPIs was selected to determine points of strengths in the current health care system in Jordan. Since the majority of study participants were on multi drug regimen, it is possible that prescribing physicians took into consideration to use the least PPIs to provoke drug- drug interaction. This may reflect a good practice by physician to protect their patients from any possible harmful interactions between medications.
This study showed that 72.5 % of participants examined did not follow current guidelines or recommendations for PPIs prescriptions. By comparing patients according to their site of care, the inappropriateness of PPIs prescription was much higher in non-ICU patient compared to ICU patients (87.4 % versus 52.4 %, respectively). Several previous studies reached a similar conclusion and have shown that there was an overuse of PPIs in different clinical settings [10,15,20-22]. Two studies conducted in a major teaching hospital in Tasmania and United kingdom, showed that inappropriate prescription of PPIs were around 60.4 % and 56.0 %, respectively [10,20]. A similar study, conducted to assess the appropriateness of PPIs prescription in patients with chronic renal failure and compared them with hospitalized patients and patients with other chronic diseases, revealed a high inadequate use of acid suppressive therapy in chronic renal failure patients (63 %) as well as hospitalized patients (81 %) compared to those with another chronic disease (32 %) [22]. More recently, it was demonstrated that 61 % of patients admitted to four different hospitals in the state of Maryland received PPIs improperly [15]. In Mexico, the prescription of PPIs was inappropriate in just 35.5 % of the cases [21].
The use aspirin or corticosteroid therapies was found among the most critical areas where PPIs were overused. For patients who required low dose aspirin for either primary or secondary prevention of cardiovascular events, both the additional risk and cost make the inclusion of PPIs unwarranted and thus inappropriate [23]. Also it is obvious from these data that physicians are still convinced in the myth of steroid ulcer, which is consistent with the result of a recent survey that showed that 82 % of physicians believe that corticosteroids are ulcerogenic [24]. However, it has been documented that the incidence of ulcer in patients receiving corticosteroids is very low. Thus, the concomitant use of anti-secretory medications is not necessary with the exception of the patients on long-term, high-dose steroids or patients on concomitant non-steroid anti-inflammatory drugs [25].
The results obtained from this study, which was conducted for the first time in Jordan, clearly demonstrate that PPIs are over-prescribed in medically hospitalized and ICU patients. This represents a major flaw in PPIs management protocols in Jordan. Sadly, the same issues that were found pertaining the PPIs therapies might be applied to other classes of pharmacologic agents and other hospitals in Jordan. Even though, additional studies are needed to better evaluate the prescription behavior of these potent acid-suppressing agents in clinical practice. In this regard, several issues have arisen that deserve further investigations. In particular, the following remain to be assessed: 1) the number of patients prescribed PPIs in relation to the total number of patients admitted to the hospital; and 2) the reasons of inappropriate PPIs prescriptions in patients with no clear indications in their medical files.
Limitations of the study
This study has a number of methodological limitations, including the retrospective nature of the survey. In addition, study data were collected only in two hospitals, and hence a multi-centered investigation may be needed to obtain results that could better reflect the prescription patterns in Jordan. It is also possible that documentation of indications for PPIs use in some medical records was not comprehensive enough in this study, which may result in overestimation of the PPIs overuse problem.
Conclusion
The current study is the first in Jordan to evaluate the prescription patterns and appropriateness of PPI therapies. The findings provide valuable information on the over-prescription of PPIs therapies in Jordan. The findings show that adherence to guidelines for safe prescription of PPIs was poor, and therefore afford a basis to establish strategies for medication management system that will improve clinical outcomes in patients on PPIs therapies. One of these strategies could be the use of a well-designed protocol that contains all the proper indications for PPIs prescribing. In addition, updating physicians’ awareness and knowledge on the appropriate indications for PPIs requires urgent attention in order to improve on healthcare systems in the country.
Declarations
Acknowledgement
References
Archives


News Updates